
Cubital Tunnel Syndrome (Ulnar Nerve Entrapment)
Cubital Tunnel Syndrome (Ulnar Nerve Entrapment) Denver, Colorado
Cubital tunnel syndrome (CuTS) is a condition I commonly treat in my hand surgery practice in the Denver metropolitan area.
CuTS is a condition of the elbow that affects the hand. It occurs when the ulnar nerve is compressed as it travels around the back of the elbow (see Figure 1). Cubital tunnel syndrome typically involves symptoms in the ring finger and small finger. It is typically felt as numbness, tingling, pain, or burning in these fingers. Think of what it feels like to ‘hit your funny bone.’ When that happens, you irritate the ulnar nerve, similar to cubital tunnel syndrome. In severe cases, CuTS can progress to irreversible weakness of the hand.
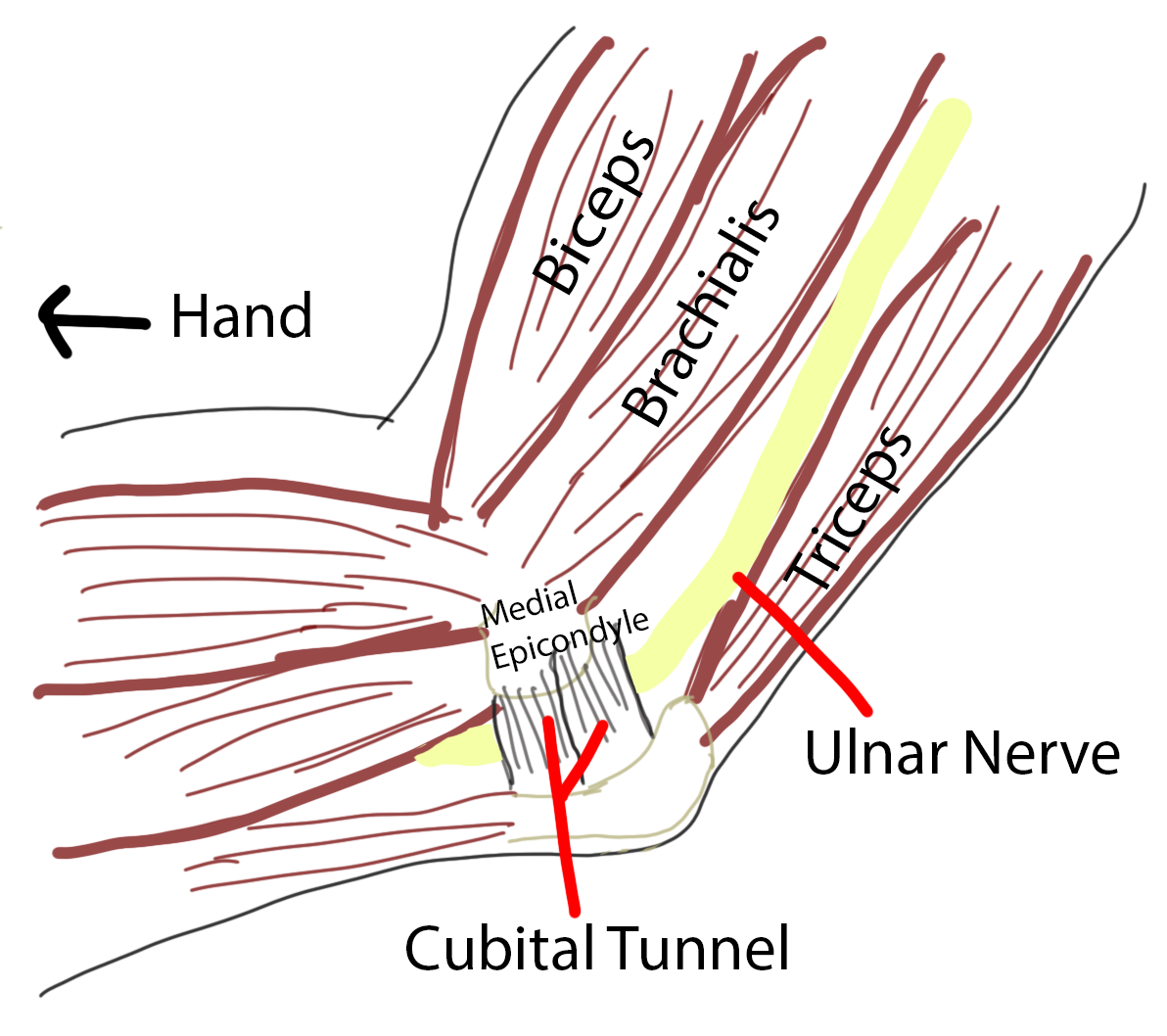
Figure 1 - In cubital tunnel syndrome, the ulnar nerve is compressed as it travels through the cubital tunnel at the elbow.
Cubital Tunnel Diagnosis & Treatment
Cubital tunnel syndrome is most often diagnosed by a detailed discussion and examination by your doctor. Occasionally, additional testing with a nerve test known as an electromyography (EMG) can be helpful. In mild to moderate forms of cubital tunnel syndrome, modifying how you use your elbow during the day can be highly effective (see below for details). In resistant forms of this condition, wearing an elbow brace at night or working with a physical therapist can also help. Patients who don’t improve with these options may wish to consider cubital tunnel release surgery.
Cubital Tunnel Release Surgery
Cubital tunnel release surgery is a relatively minor procedure with a high rate of success. In this surgery, I make a 4 to 5-cm incision at your inner elbow to reveal the cubital tunnel compressing the ulnar nerve. After dividing the tunnel, your nerve will no longer be compressed. In about 10% of cases, the ulnar nerve is unstable at the back of the elbow so I formally move it to the front of the elbow in a procedure known as an ‘anterior transposition.’
Additional Information
If you’d like more information on cubital tunnel syndrome, please continue reading through my patients’ frequently asked questions below. You may also navigate to my ‘deep dive’ section to the right of the FAQs where I have links to the longer-form articles I have written about cubital tunnel syndrome and its treatment.
Rules of Thumb Newsletter
Dr. G's simple, actionable weekly guides to combat the injuries, aches, and pains of the hand and upper extremities.
The Basics
-
Cubital Tunnel Syndrome is a collection of symptoms that result from compression of the ulnar nerve in the cubital tunnel. The cubital tunnel is an anatomic space around the back of the elbow through which the ulnar nerve passes as it travels down the arm (see Figure 1).
Have you ever hit your funny bone? Hitting your funny bone is actually a direct strike on your ulnar nerve as it courses around the back of your elbow. You can even think of this as ‘acute’ cubital tunnel syndrome!
-
Cubital tunnel syndrome results when there is any compression on the ulnar nerve inside the cubital tunnel. The ulnar nerve passes around the back of your elbow and can be compressed at many points along this path (see Figure 1).
What is different about cubital tunnel syndrome, rather than carpal tunnel, is that cubital tunnel is most often caused by dynamic compression of the ulnar nerve at the elbow. This means that the nerve moves in and out of compression, depending on the position of your arm. Any time your elbow is bent 90° or more, the ulnar nerve will be compressed behind your elbow. Prolonged periods of elbow bending, common in modern activities like typing, reading, and texting, contribute to constant nerve compression.
-
Anyone can develop cubital tunnel syndrome. But those who engage in activities involving prolonged elbow flexion, such as typing, texting, or leaning directly on the elbow (think desk chair or console while driving), are at a higher risk.
Our 21st-century lives require increased time spent in positions that compress the ulnar nerve, and I suspect this may lead to a higher prevalence of cubital tunnel syndrome over time.
Cubital Tunnel Symptoms & Diagnosis
-
Cubital tunnel symptoms include numbness and tingling in the ring and small fingers. These symptoms can also include pain or burning and often involve both the palm side and back side of the fingers.
In severe cases, patients can permanently lose the muscle mass between their hand bones and suffer from irreversible weakness of the hand, particularly with fine motor tasks.
-
Currently, the standard diagnosis of cubital tunnel syndrome is by a detailed discussion with your doctor and a physical examination. Cubital tunnel syndrome can be confused with other conditions, and in these cases, nerve tests known as electromyography or nerve conduction studies (EMG/NCS) can be helpful. This is a test performed by a neurologist.
Unfortunately, there is a high rate of ‘false-negative’ results with EMG testing in cubital tunnel syndrome. This occurs because ulnar nerve compression is often dynamic (see above ‘What causes cubital tunnel syndrome?’), yet the test is performed with the elbow straight. In this way, the test can mistakenly miss ulnar nerve compression at the elbow.
Because of this, there is fervent interest in additional testing modalities. The most promising is the use of ultrasound to measure the cross-sectional area of the ulnar nerve at the elbow. More to come in this realm!
-
While most patients would not describe the test as frankly painful, it can be uncomfortable to some. The test involves transmission of a small electrical current through the arm to measure the speed at which electricity is conducted down the ulnar nerve through the cubital tunnel.
-
Because this test is conducted by a neurologist, it will require a referral. This is a referral we can send to a local facility. That office will contact you to arrange a time and location for your nerve test.
Cubital Tunnel Treatment
-
If you’re interested, I go into this in more detail in my deep dive “What Is Cubital Tunnel Syndrome? The Ultimate Patient Guide”
If you think you have cubital tunnel syndrome, the first thing to do is take a careful inventory of your daily activities. Do you spend periods of the day in prolonged elbow flexion? Think typing, texting, watching TV or reading with your head resting on your hand, driving, etc.
Then see if you can take steps to eliminate or shorten these periods. If you can’t, at the very least take regular breaks where you let your arm hang down in a straighter position. This allows your ulnar nerve to ‘un-pinch’ for a few moments. If you can make these changes consistently for 3-4 months, you are likely to cure your symptoms.
Nighttime bracing, which prevents excessive elbow flexion during sleep, can also be highly effective. See my article linked here for a step-by-step guide to making your own cubital tunnel night splint.
-
Physical therapy can be beneficial for cubital tunnel syndrome in some cases. Stretching exercises and nerve glides may help balance overall nerve tension, particularly if this is the root cause of your compression. While by no means a cure-all, therapy may be worth trying if the at-home solutions are not helping with your symptoms.
-
Steroid injections are not a mainstay of cubital tunnel syndrome treatment. Long-term symptom relief has yet to be shown reliably in scientific studies. Additionally, there is a risk of nerve injury with this type of injection.
An injection may occasionally be used under image guidance (eg, ultrasound) to help diagnose cubital tunnel syndrome if the diagnosis is unclear. In this setting, immediate relief of symptoms following injection can help uncover a confusing diagnosis, even if the relief is temporary and short-term. This way of using a cubital tunnel injection has in fact been shown to reliably predict which patients would benefit from cubital tunnel release surgery.
Cubital Tunnel Surgery
-
The surgery for cubital tunnel syndrome is called a cubital tunnel release. In this procedure, a 4-5cm incision is made on the inner elbow, and the cubital tunnel is identified. All areas of compression around the ulnar nerve are relieved with this procedure.
-
In about 10% of cases, the ulnar nerve becomes ‘unstable’ at the back of the elbow following standard release. This is typically a finding we can only identify in surgery after the initial release. In some cases, a patient comes to my office with nerve instability that can be felt on examination.
In cases of nerve instability, whether pre-operatively or after standard release, the typical practice is to perform an anterior transposition. In this procedure, the purpose is to remove the nerve from a setting where it will flip back and forth over the inner elbow with elbow flexion. This can be very painful and will result in continued cubital tunnel symptoms.
Instead, the nerve is moved to the front of the elbow, and secured in the tissues in this new location.
-
If you have obvious snapping at the inner elbow when you bend your elbow, along with your cubital tunnel symptoms, you may benefit from a nerve transposition.
More commonly, I directly visualize nerve instability during a standard cubital tunnel release and then make the decision to transpose the nerve based on this intra-operative finding. This occurs in about 10% of all cubital tunnel release surgeries.
-
To me, this is the cornerstone of understanding nerve elease surgery. The only thing we can do as surgeons is release the pressure on your ulnar nerve. This allows the restoration of blood flow and nutrients.
Once this happens, the nerve begins a biological healing process. This, unfortunately, is a process you and I have no control over. Your nerve is going to work to heal itself, but the degree to which this occurs is out of our control.
Nerves that have been compressed more severely or for a longer duration have the hardest time recovering. Here’s a summary of what I typically see:
The vast majority of patients have a resolution of their painful nerve symptoms (burning, tingling, pain).
Many have full restoration of their sensation. However, some patients suffering from ulnar nerve compression show little improvement following cubital tunnel release surgery.
Very few patients have any improvement of weakness or muscle loss from prolonged nerve compression. This is typically irreversible.
If you’ve seen me for cubital tunnel syndrome, then you know I stress this a lot:
Cubital tunnel release surgery is performed so that your symptoms won’t continue to worsen; improvement following release is common, but by no means guaranteed.
I find it helpful to understand the biology when developing expectations around cubital tunnel release surgery.
-
Cubital tunnel release surgery is a day surgery typically performed in an outpatient surgery center. This is typically performed under a light anesthetic.
In this procedure, patients receive a ‘twilight’ sedation (similar to a wisdom tooth extraction or colonoscopy procedure) during which they feel asleep but are breathing on their own without the need for a breathing tube.
-
Following cubital tunnel release surgery, you will have absorbable sutures in your elbow. These do not need to be removed.
All my patients have a visit with a Certified Hand Therapist within 10-14 days of surgery. They will examine your incision and begin gentle exercises. If you’ve had a transposition, they will make you a temporary custom splint while your nerve heals in its new location. Any concerns are communicated directly to me by my team.
I will then meet with you approximately 3 weeks after surgery to evaluate your healing process. Many patients are healed and nearly ready for release from care at that time. I typically allow a return to heavy lifting around 4 weeks. If you’ve had a transposition, I will continue to limit your heavy lifting activities for a minimum of 6 weeks while your nerve heals in its new location.
-
Restrictions are fairly simple after cubital tunnel release surgery. The surgical dressing must stay on and dry for the first 5 days after the procedure. Finger movement and light to moderate use of the hand and wrist is allowed and encouraged. But you must take care not to do anything vigorous enough to tear the stitches or disrupt wound healing.
In a standard cubital tunnel release surgery, gentle elbow motion begins right away. I ask you to avoid heavy lifting for the first 4 weeks. If you have had a transposition, there is a short period of splinting followed by heavy lifting restrictions for 6 weeks.
-
Fortunately, the risks of cubital tunnel surgery are low. Any surgery has risks associated with anesthesia, pain, bleeding, and infection. Additionally, there is a very small risk of nerve injury. Some patients do not improve (see more above) or have a recurrence of their cubital tunnel syndrome in the future.
-
Ultimately, your decision for surgical treatment of cubital tunnel syndrome is just that - your decision.
If your cubital tunnel syndrome is mild to moderate in severity, it can be a reasonable decision to avoid or delay surgery. If you make this decision, you must understand that many cases of cubital tunnel syndrome slowly worsen over time. And they can worsen to the point of permanent muscle loss in the hand. So if you decide no surgery for now, be sure to follow up with your hand surgeon every 6 months to ensure your symptoms aren’t progressing beyond a point of no return.
In the case of severe cubital tunnel syndrome, the standard recommendation will be for surgical release as soon as possible. Severe cubital tunnel syndrome means the muscles in your hand are no longer receiving adequate signals from the ulnar nerve. These muscles will eventually shrink (atrophy) and eventually disappear. This is an irreversible condition that can result in a dysfunctional hand.

